Lunate / Perilunate Dislocation
YOU HAVE ONE MINUTE TO READ THE FOLLOWING CLINICAL SCENARIO:
You’re the Ortho SpR on call. One of the A+E consultants phones you for some advice regarding a patient that was reviewed earlier in the department.
The patient sustained a fall onto an outstretched left hand whilst running. He had radiographs taken that didn’t show any fractures. Since the gentleman was still complaining of pain in the wrist he was given a futuro splint and discharged with a fracture clinic appointment. Apart from a few minor cuts and lacerations, the patient sustained no other injuries.
The A+E consultant is reviewing the radiographs from the morning and would like a second opinion regarding the X-ray.

Always start with the patient demographics. Although given in this instance, always ask for another (usually orthogonal) view if you are presented with only one. Do first describe the x-ray given to you though.
This is an AP and lateral of a patient’s left wrist taken at….. I can see no fractures. However there is carpal malalignment and disruption of Gilula’s lines, suggestive of a peri-lunate dislocation.
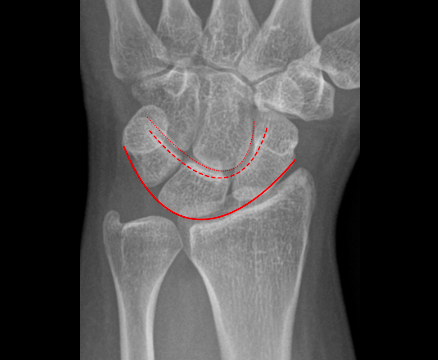
When reviewing an X-ray with respect to the carpus, there are 3 lines that are reviewed (Gilula’s three carpal arcs). They are used to asses alignment of the carpal bones on an AP radiograph.
In addition the distal radius, lunate and capitate should all be in linearity with one another on the lateral radiograph.
Gilula’s Carpal arcs:
- 1st arc – In a normal radiograph this should be a smooth line between the proximal convexities of the scaphoid, the lunate and the triquetrum
- 2nd arc – same as the 1st arc but looking at the distal outline of these bones.
- 3rd arc – this should be a smooth line along the proximal ends of the capitate and the hamate
AP Radiographic findings for a peri-lunate dislocation are:
- discontinuity in any one of the carpal arcs
- overlapping of the lunate and the capitate
- triangular appearance of the lunate known as the ‘piece of pie’ sign
Lateral radiographic findings are:
- loss of linearity between the radius, lunate and capitate
- a scapho-lunate angle of greater than 70 degrees (angle between two lines that bisect the scaphoid and lunate respectively into 2)
Peri-lunate dislocations require URGENT reduction. Approximately 25% are missed on first presentation.
This peri-lunate dislocation requires urgent reduction. I would therefore inform the A&E consultant of the diagnosis and ask him to contact the patient and arrange for him to return to hospital immediately. I would also ask the consultant to ensure that the patient did not have anything further to eat or drink. I would then discuss the x-ray and proposed further management with my consultant.
Essentially, it’s important that you convey to the examiner that you know this is an urgent/emergent situation. starting off the answer with something to that effect will again put the examiner at ease.
Peri-lunate dislocations require URGENT reduction. Approximately 25% are missed on first presentation.
This peri-lunate dislocation requires urgent reduction. I would therefore inform the A&E consultant of the diagnosis and ask him to contact the patient and arrange for him to return to hospital immediately. I would also ask the consultant to ensure that the patient did not have anything further to eat or drink. I would then discuss the x-ray and proposed further management with my consultant.
Essentially, it’s important that you convey to the examiner that you know this is an urgent/emergent situation. starting off the answer with something to that effect will again put the examiner at ease.
This question requires a small amount of knowledge but is predominantly management based. Closed reduction of peri-lunate dislocations is possible but most will require an open reduction.
It is therefore completely reasonable to attempt a reduction in A+E when the patient arrives (which is what would normally have happened if the patient had not left the department) but you need to be prepared and aware that you will probably have to take the patient to theatre and perform an open reduction. The patient should also be made aware of this.
“I would review this patient in the A+E department and perform a thorough examination documenting any neurological deficits. I would then plan to reduce the dislocation in the A+E department under sedation and relaxation. I would inform my consultant before attempting this as there is a high probability the patient may ultimately require an open reduction.”
Interposing capsule will usually be the culprit blocking a closed reduction – but in any case the soft tissues need to be relaxed. This can be achieved using finger traps and hanging the patient’s arm out at 90 degrees elbow flexion for a period of 10-15 minutes.
Tavernier’s manoeuvre describes thumb pressure to the lunate and traction to the fingers to create a space for the lunate, followed by wrist extension (to exaggerate the dislocation) and then flexion to reduce the proximal capitate. After attempted closed reduction, neurovascular status should be re-checked.
“I would then put the patient into finger traps on the affected side and hang the patient’s arm from a stand with the elbow flexed at 90 degrees to relax the soft tissues for approximately 15 minutes. I would ask my A+E or anaesthetic colleagues for sedation and muscles relaxation and then attempt a closed reduction after informing my consultant. I would apply traction, extend the wrist and then flex the wrist to reduce the dislocation. I would then recheck neurovascular status and ask for a repeat X-ray.”
As mentioned before, closed reduction to these injuries is often unsuccessful and recurrent dislocation can occur with older in injuries. It is important to establish that open reduction is urgent if there is any indication of an acute median nerve palsy.
It is not important to know the in-depth steps of surgical repair but rather the principles and safe management of this injury.
“I would escalate this patient to the consultant as they will require an open reduction in theatre. I would ensure the patient is appropriately marked, consented and starved for the next available trauma theatre slot. I would complete all appropriate pre-operative investigations including blood tests and ECG. I would inform on-call anaesthetists and theatre staff.
This patient will require open reduction, possible ligament repair or fixation and possible carpal tunnel release”
In a peri-lunate dislocation the entire carpus ‘falls’ backwards whilst the lunate stays in it’s normal anatomical position.
In a lunate dislocation the lunate is forced from its normal anatomical position whilst the carpus remains undisplaced.
The Mayfield Classification describes carpal ligamentous injuries.. It describes the different ligamentous injury/instability that is sustained with progressive disruption and instability:
1) Scapholunate dissociation
2) Scapholunate dissociation+lunocapitate disruption
3) Scapholunate dissociation+lunocpitate disruption + lunotriquetral disruption (a perilunate dislocation)
4) Lunate dissociated from the lunate fossa – usually displaces in a volar direction and highest incidence of median nerve compression (a lunate dislocation)